전립선비대증 수술 후 우연히 발견된 전립선암의 진단과 치료방법에 대한 고찰
1. Introduction
2. Incidence of Incidental Prostate Cancer
3. Active surveillance
4. Active Surveillance program
5. Consideration for treatment of patients on Active Surveillance
6. Treatment option
7. Conclusion
1. Introduction
우연히 발견되는 전립선암(IPCa, incidental prostate cancer) 이란 증상이 없거나 직장수지검사(DRE)에서 만져지지 않았으나, 전립선비대증 수술 후 우발적으로 발견된 종양을 뜻합니다 [1]. 병리학적 T stage에선 정의에 따라 pT1가 존재할 수 없기 때문에 2023년 NCCN guideline에선 clinical stage T1에 포함시키고 있으며 [2], 2023년 EAU guideline에선 잘려진 (resected) 조직에서 ISUP (International Society of Urologic Pathologists) grade 1이 5% 이하일 경우엔 cT1a, 5% 초과일 경우엔 cT1b로 소개하고 있다. Stage의 경우 AJCC prognostic groups에서 PSA level에 따라 Stage I 부터 Stage IIA에 포함에 있다.
문헌들에서 IPCa가 진단되는 전립선비대증 수술은 조직의 확인이 가능한 경요도적전립선절제술(TUR-P)이나 홀렙(HoLEP)을 주로 언급하고 있으나, 최근엔 로봇을 이용한 단순전립선적출술(Robot assisted-simple prostatectomy)도 포함될 수 있겠다.
하지만 전립선비대증 수술에서 절제영역은 주로 전환대(transition zone)이며, 말초대(peripheral zone)의 임상적으로 유의미한 전립선암(clinically significant prostate cancer)의 발견을 간과할 수 있다. 또한 전기소작(electro-cauterization)으로 인해 발생하는 아틱팩트(artifact)도 고려해야하고 무엇보다 가이드라인상의 “5%”가 잘려 나온 전체 전립선조직 중 양성칩(positive chip)의 퍼센트를 뜻하는 것인지, 아니면 확인된 전립선암이 차지하는 부분(proportion of cancer)을 뜻하는 것인지가 모호할 수 있다. 추가로 IPCa가 공격적으로 악화되는 증례들이 보고되고 있어 [3], 가이드라인상 IPCa의 영역을 더욱 넓혀야 한다는 의견들이 회자되고 있다 [4].
이에 전립선비대증 수술 후 우연히 발견된 IPCa의 진단, 능동감시와 치료에 대해 최신 지견을 정리해보고자 한다.
2. Incidence of Incidental Prostate Cancer
교과서적으로 새로 진단되는 전립선암 환자 중 촉진되지 않는 경우는(AJCC cT1c) 약 60-70%라고 알려져 있다 [5]. 2018년 P Capogrosso등은 1177명의 비대증수술 환자 중 약 6.4%의 유병율을 보였으며, 비대증수술 전 전립선조직검사를 시행한 군에서 IPCa 발견률이 유의하게 낮았다고 하였다. 반면 지난 10년간 IPCa의 발생율이 상승하였는데, 그 이유로는 PSA가 높은 군에서 prostate MRI 촬영의 빈도수가 늘면서 무분별한 전립선생검의 감소로 보고 있고, 증가한 IPCa는 대부분 low grade (Gleason score 6)이기 때문에 긍정적인(favorable) 종양학적 결과를 보인다고 주장하였다 [6]. 이는 HU Ahmed등의 PROMIS study와 유사한 결론이다 [7]. 2022년 BKC Cheng등은 55개의 연구를 이용한 메타분석에서 IPCa의 빈도를 약 8%로 발표하였다. 나이, 비대증수술 전 PSA level과 PSA density, 전립선크기가 작을수록 그리고 비대증수술 후 PSA 상승속도가 빠를수록 IPCa의 발견율과 유의하게 연관 있었다고 하였다 [8]. 2022년 Zhelang Guo등이 메타분석을 통해 94,783개의 전립선비대증 수술 환자 중 24,715명의 IPCa 환자가 진단되어 약 26.1%의 가장 높은 유병율을 보고하기도 하였다 [9]. [그림 1]은 나이에 따른 IPCa의 발병율을 보여준다.
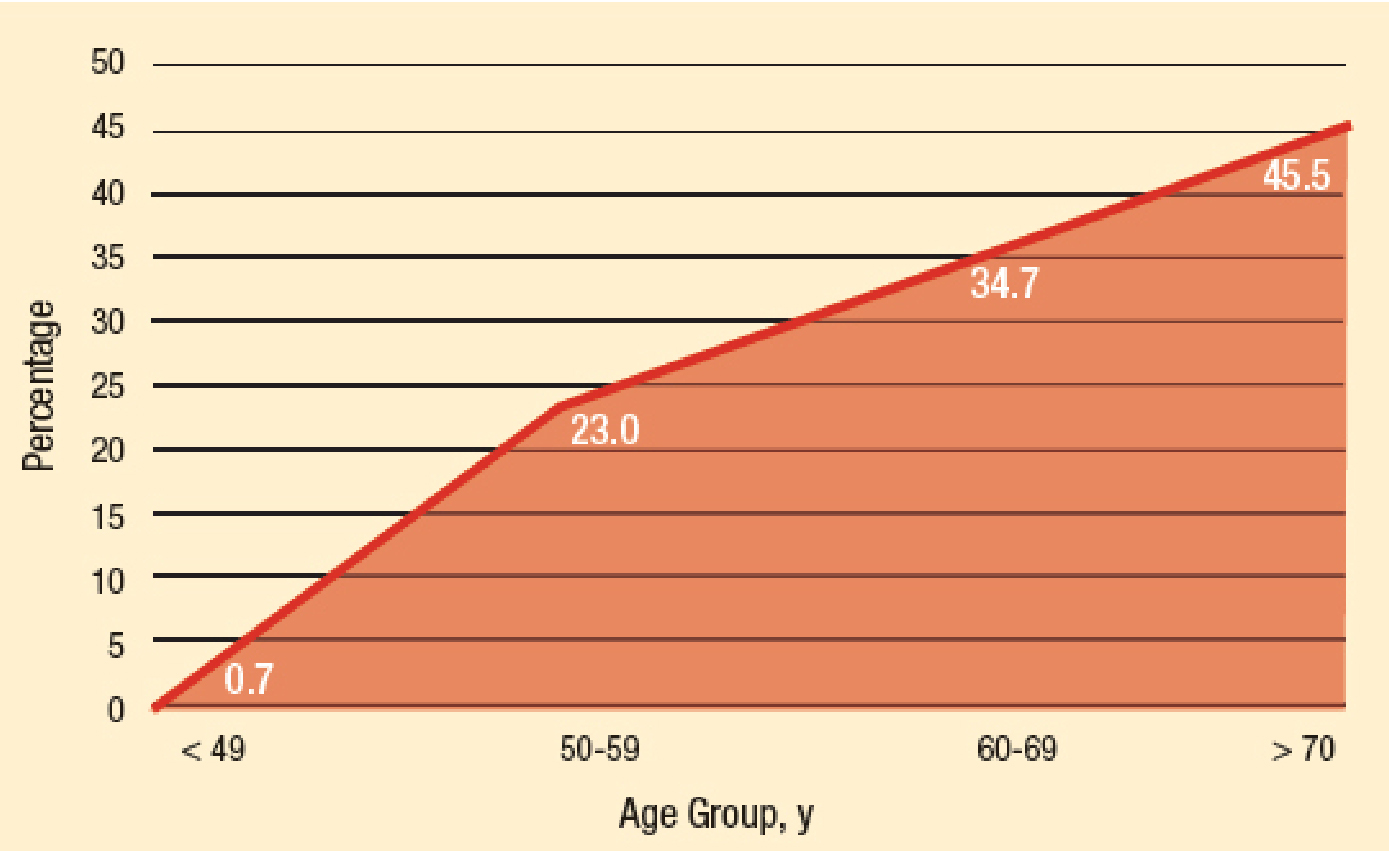
그림 1.
Prevalence of Incidental Prostate Cancer by age [13]
방광암으로 근치적방광적출술 후 발견되는 IPCa의 경우 유병율이 약 20%로 보고되었으며, 이중 15%는 ISUP grade 1, 3.2%는 grade 2, 1.2%에서 grade 3가 확인되었다고 한다. 10년 생존률은 전립선암에선 99%, 방광암은 57%이었다 [10].
전립선비대증 수술 전 인자들 중 IPCa 발견율과 연관 있는 것으론 PSA가 대표적이며, 이외에 전립선 크기와 나이가 연관이 있다고 [11] 하지만, PSA만이 유일한 위험요인으로 발표한 연구도 있다 [9].
지금까지의 가이드라인들은 전립선암을 위험도(risk stratification)에 따라서 치료 방침을 결정하는데 IPCa의 경우 cT1a/b에 포함되기 때문에 low risk로 판단 한 뒤 능동감시 또는 감시대기요법 정도로 짧게 정리하고 있다. 이에 IPCa에 대해 비뇨의학과 의사들의 보다 많은 관심과 연구가 필요하다고 제기되고 있다 [12].
3. Active surveillance
NCCN guideline의 Pros-F 2of 5를 보면 능동감시의 적절성 평가를 위해 최초 조직검사 이후 확증성 시험(confirmatory testing)을 권유하고 있다. 이는 과소평가될 수 있는 종양에 대해 6개월에서 12개월내에 PSA density 계산과 더불어 mpMRI 촬영 및 molecular tumor analysis등의 추가 검사를 시행하는 것을 뜻하며, 특히 능동감시 중인 모든 환자는 최초 조직검사 날로부터 1-2년째에 재조직검사(confirmatory biopsy)할 것을 권유하고 있다. 한국의 경우 능동감시시 생화학적재발이 없는 생존율(biochemical recurrence free survival)은 T1a에서 93%, T1b에서 70%로 차이를 보였다고 한다 [14].
4. Active Surveillance program
능동감시 중 임상적으로 필요하지 않다면, PSA는 6개월 이상의 간격을 두고 시행하며 직장수지검사는 12개월 이상의 간격을 두고 시행해볼 수 있다. Confirmatory biopsy 이후의 재조직검사(repeat biopsy)는 12개월 이상의 간격을 둘 수 있으며, mpMRI는 12개월 이상의 간격을 두고 시행할 것을 권유하고 있다. 기대여명이 10년 미만으로 예상되는 경우 경과관찰(observation)로 전환할 수 있으며 molecular tumor analysis를 재검사하는 것은 의미가 없다.
5. Consideration for treatment of patients on Active Surveillance
능동감시 중 치료가 필요한 상황으로는 재조직검사에서 ISUP grade가 상승하는 경우가 가장 빈도가 높으며 [15], 종양의 부피 증가, PSA 농도의 상승 그리고 환자의 불안감 등이 원인이 되기도 한다. 능동감시에서 경과관찰 또는 치료로 대응 방법이 달라질 때는 환자의 기대여명을 꼭 고려해보아야 하겠다. 절제조직에서 확인된 종양의 grade에 따라 치료 방침을 결정하자는 의견도 있으며, ISUP grade가 2가 확인되었을 땐 6-8주 이후에 mpMRI 촬영 및 말초대에 대한 조직검사를 제시하였다. ISUP grade가 더 높은 경우엔 능동감시는 더 이상 유효하지 않는다 [4].
6. Treatment option
2023년 Klein등은 IPCa의 유병율을 약 10.7%로 보고하였으며, 비대증 수술 후 cT1b와 PSA>2ng/mL인 경우 더 높은 진행(higher progression)을 보였다고 하였다 [12]. TUR-P 수술 후 근치적전립선적출술의 실현 가능성(feasibility)는 과거에 요실금의 회복이 더디고 출혈이 많으며 요누출등의 합병증 발생율이 높다는 보고들이 많았다 [16]. 하지만 다빈치 시스템과 같은 로봇장비의 도입으로 TUR-P수술 후 로봇근치적전립선적출술(RARP)을 진행함에 있어 발생하는 요실금은 TUR-P를 시행하지 않은 군과 유의미한 차이가 없었고 오히려 절제면 양성률(positive surgical margin)은 낮았기 때문에 충분히 실현 가능하다고 발표한 연구들이 있다 [17,18]. HoLEP 수술의 경우 RARP 수술을 진행하는데 있어 bladder neck reconstruction 때문에 시간이 더 오래 걸릴 수 있으며 성기능 회복이 더디었지만, 절제면 양성률은 대조군에 비해 적었으며 생화학적재발율과 요실금 회복은 유의한 차이가 없었다고 한다 [19].
방사선치료(External radiotherapy, RT)의 경우 전립선비대증 수술 후 발견된 IPCa환자에게 적절한 삶의 질을 제공할 수 있다고 한다. RT로 인한 배뇨독성(urinary toxicity)는 TUR-P수술을 하지 않은 군과 차이가 없이 발생하였으나, 최근 Intensity Modulated Radiotherapy(IMRT)의 발전으로 장기간 관찰하였을 때 배뇨독성은 사라졌다고 발표하였다 [20].
2021년 J Herden등은(HAROW study) 능동감시를 하던 IPCa환자들 중 33.8%가 병의 진행으로 치료를 시작하였는데, 12명은 근치적전립선적출술, 7명은 방사선치료, 4명은 호르몬 치료(Hormone therapy)를 선택하였으며 IPCa로 인한 사망(cancer specific death)는 없었다고 보고하였다 [21].
7. Conclusion
IPCa의 유병율은 보고된 기관마다 차이는 있으나 5-14%정도로 파악되며, 능동감시 또는 치료 여부 결정은 기대여명, PSA level 그리고 병리학적 기수가 중요하겠다. IPCa의 진단과 치료방침은 가이드라인에 새로운 목차를 만들어 줄 수 있는 영역이며, 무엇보다 의료진과 환자가 충분한 의논을 한 후 치료방침을 결정하는 것이 선호되겠다.
Editorial Comment
전립선비대증 수술로 우연히 발견되는 전립선암은 의사와 환자 모두에게 중요한 문제이다. 전립선비대증 수술 후 발견되는 전립선암은 일반적으로 초기 단계에 있을 확률이 높으나, 정확한 평가와 적절한 치료 계획이 필수적이다. 비뇨의학과, 종양내과, 방사선종양학과 등 다학제적 접근 방식이 중요하며, 환자의 개별적인 상황을 고려하는 것이 중요하다. 이는 암의 병기, 환자의 전반적인 건강 상태, 그리고 환자의 선호도와 추가 치료에 대한 기대치를 포함하게 된다. 일부 경우에는 능동감시가 최선의 선택일 수 있으며, 다른 경우에는 적극적인 치료가 필요할 수도 있다. 이와 함께 전립선비대증 수술 후 발견되는 전립선암의 사례는 전립선암의 조기 발견과 예방에 대한 중요성을 시사한다. 전립선비대증 환자들의 정기적인 전립선암 검사가 중요하고, 이는 우연히 발견되는 전립선암의 조기 발견과 적절한 환자 관리에 중요한 역할을 한다고 할 수 있다.
전립선비대증의 유병률과 진료가 증가하는 만큼, 전립선비대증 수술 후 우연히 발견되는 전립선암은 비뇨의학과의 중요한 이슈이며, 전립선암의 진단과 치료에 있어 환자에 따른 개별적인 접근이 필수적이고, 조기 발견과 예방적 활동에 대한 노력이 중요하다고 할 수 있다. 다양한 연구자료를 일목요연하게 정리해준 저자께 감사드린다.
References
Abedi A-r et al., Incidental prostate cancer: a 10-year review of a tertiary center, Tehran, Iran. Research and reports in urology, 2018
10.2147/RRU.S14615929392121PMC5768285Moses KA et al., NCCN Guidelines® Insights: Prostate Cancer Early Detection, Version 1.2023: Featured Updates to the NCCN Guidelines, Journal of the National Comprehensive Cancer Network, 2023
Robinson D et al., Long-term follow-up of conservatively managed incidental carcinoma of the prostate A multivariate analysis of prognostic factors, Scandinavian journal of urology and nephrology, 2007
10.1080/0036559060099126817454947Mottet N et al., Incidental prostate cancer: a real need for expansion in guidelines? European Urology Oncology, 2022
10.1016/j.euo.2021.04.00634020930Partin AW et al., Campbell Walsh Wein Handbook of Urology: Campbell Walsh Wein Handbook of Urology-E-Book: Elsevier Health Sciences, 2021
Capogrosso P et al., Temporal trend in incidental prostate cancer detection at surgery for benign prostatic hyperplasia, Urology, 2018
10.1016/j.urology.2018.07.02830138683PMC6724539Ahmed HU et al., Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study, The Lancet, 2017
10.1016/S0140-6736(16)32401-128110982Cheng BK-C et al., Incidence, predictive factors and oncological outcomes of incidental prostate cancer after endoscopic enucleation of the prostate: a systematic review and meta-analysis, World Journal of Urology, 2022
10.1007/s00345-021-03756-934142230Guo Z et al., Prevalence and risk factors of incidental prostate cancer in certain surgeries for benign prostatic hyperplasia: A systematic review and meta-analysis, International braz j urol, 2022
10.1590/s1677-5538.ibju.2021.065335195386PMC9747035Packiam VT et al., Long-term outcomes of incidental prostate cancer at radical cystectomy. In: Editor, editor.^editors. Book Long-term outcomes of incidental prostate cancer at radical cystectomy. Series Long-term outcomes of incidental prostate cancer at radical cystectomy. 38: Elsevier, 2020
10.1016/j.urolonc.2020.05.01832624422Mohamed AH et al., Incidence and associated factors for incidental prostate cancer among patients who underwent surgery for benign prostatic hyperplasia: first report from Somalia, Journal of Cancer Research and Clinical Oncology, 2023
10.1007/s00432-022-04319-036036824PMC10314863Khan FA et al., Current Trends in Incidence and Management of T1a and T1b Prostate Cancer, Cureus, 2023
10.7759/cureus.40224Chin HW et al., Prostate Cancer in Seniors: Part 1: Epidemiology, Pathology, and Screening, Federal Practitioner, 2015
Lee DH et al., Clinical experiences of incidental prostate cancer after transurethral resection of prostate (TURP) according to initial treatment: a study of a Korean high volume center, Yonsei medical journal, 2014
10.3349/ymj.2014.55.1.7824339290PMC3874906Han JH et al., Natural history of incidentally diagnosed prostate cancer after holmium laser enucleation of the prostate, Plos one, 2023
10.1371/journal.pone.027893136730281PMC9894415Li H et al., Radical prostatectomy after previous transurethral resection of the prostate: a systematic review and meta-analysis, Translational Andrology and Urology, 2019
10.21037/tau.2019.11.1332038968PMC6987598Suardi N et al., Nerve-sparing radical retropubic prostatectomy in patients previously submitted to holmium laser enucleation of the prostate for bladder outlet obstruction due to benign prostatic enlargement, European urology, 2008
10.1016/j.eururo.2007.07.02717659829Tappero S et al., Retzius-sparing robot-assisted radical prostatectomy after previous trans-urethral resection of the prostate: Assessment of functional and oncological outcomes, European Journal of Surgical Oncology, 2023
10.1016/S0302-2838(23)00538-9Abedali ZA et al., Robot-assisted radical prostatectomy in patients with a history of holmium laser enucleation of the prostate: the Indiana University experience, Journal of Endourology, 2020
10.1089/end.2019.043631822128Ishiyama H et al., Is there an increase in genitourinary toxicity in patients treated with transurethral resection of the prostate and radiotherapy?: a systematic review, American journal of clinical oncology, 2014
10.1097/COC.0b013e318254682122706173Herden J et al., Active surveillance for incidental (cT1a/b) prostate cancer: long-term outcomes of the prospective noninterventional HAROW study, Urologia internationalis, 2021
10.1159/00051289333517336
