
1. 서론
방광통증후군/간질성방광염 (Bladder pain syndrome/interstistial cystitis; BPS/IC)은 그동안 용어와 정의, 진단기준 등에서 많은 혼동과 변화가 있어왔다. 지금까지 많은 노력과 연구들이 있었지만 아직도 어느 것 하나 명확히 규정된 것은 없다고 해도 과언이 아닐 것이다. 2002년 International Continence Society (ICS)에서는 painful bladder syndrome/interstitial cystitis라는 용어를 사용하였으며, 요로감염이나 다른 명백한 병인이 없이 방광의 충만과 함께 발생하는 치골 상부의 통증으로 주간 및 야간 빈뇨를 동반하는 경우로 정의하였다 [1]. 이후 European Society for the Study of Interstitial Cystitis (ESSIC)에서는 bladder pain syndrome이라는 용어를 사용하기로 하고 급박뇨나 빈뇨와 같은 배뇨 증상이 적어도 하나 이상 동반하는 방광과 관련된 만성 골반 통증, 압박감 또는 불편감이 있을 때 진단하는 것으로 규정하였다 [2].
최근에는 BPS/IC의 진단은 다른 질환들을 배제하면서 임상 증상과 함께 특징적인 방광경소견과 조직학적소견이 동반되어야 한다고 의견이 우세하다. 하지만 아직도 어느 범위까지를 BPS/IC로 봐야하는가에 대한 진단기준이 불명확한 현 상태는 계속 문제점으로 남아있으며 이로 인해 효과적인 치료법 또한 제시하기 어려운 실정이다. BPS/IC의 진단과 치료에 대해 최신 문헌고찰을 통하여 살펴보고자 한다.
2. 본론
2.1. 진단
아직까지도 BPS/IC에 대한 임상 증상과 진단기준은 불명확하다 [3], [표 1].
표 1. Comparison of contemporary definitions of BPS/IC
통증은 BPS/IC의 가장 특징적인 증상이다. 전형적인 통증 양상은 방광의 충만과 함께 발생하는 치골 상부의 통증, 압박감 또는 불편감뿐만 아니라 요도, 외음부, 질, 직장에 걸친 골반 통증과 하복부와 등 부위와 같은 골반 이외의 부위에서도 통증을 호소한다. 또한 BPS/IC 환자들은 급박뇨나 빈뇨와 같은 배뇨 증상을 호소한다. 이러한 경우 과민성방광과 구별해야 하는데, BPS/IC 환자들은 방광의 충만과 함께 동반되는 통증을 피하거나 줄이기 위해 배뇨하는 반면에, 과민성방광 환자들은 요실금을 피하기 위해 배뇨를 한다는 점이다.
증상을 확인한 이후에는 그 같은 증상을 일으킬 수 있는 질환들을 진단하거나 배제해야 한다. 감별해야하는 질환들로는 만성 요로감염, 요도 게실, 과민성방광과 골반 통증을 유발할 수 있는 다른 질환들, 예를 들면 자궁내막증, 외음부 통증, 질 칸디다증 등이 있다 [4]. 이렇게 다른 질환들을 배제하고 BPS/IC로 진단되면 방광경검사 소견과 방광조직검사 소견에 따라 분류한다 [5], [표 2].
표 2. Classification of interstitial cystitis and interstitial cystitis-related conditions in different guidelines
방광내시경은 진단에 있어서 증상을 일으킬 수 있는 방광암, 자궁내막증, 감염 또는 방광결석과 같은 질환들을 배제하기 위해 권고되며 구상화 병변 (glomerutation)과 Hunner 궤양과 같은 특징적인 방광경 소견을 나타내는 경우도 있다 [5], [그림 1]. 그리고 방광 조직검사을 통해 요상피세포의 손상, 만성 염증 비만세포의 군집과 같은 조직학적 소견이 확인되는 경우도 있다 [6,7]. 그러나 이러한 병인이 BPS/IC 진단에 도움이 될 수는 있으나, BPS/IC에 특징적인 조직학적 소견은 없다.
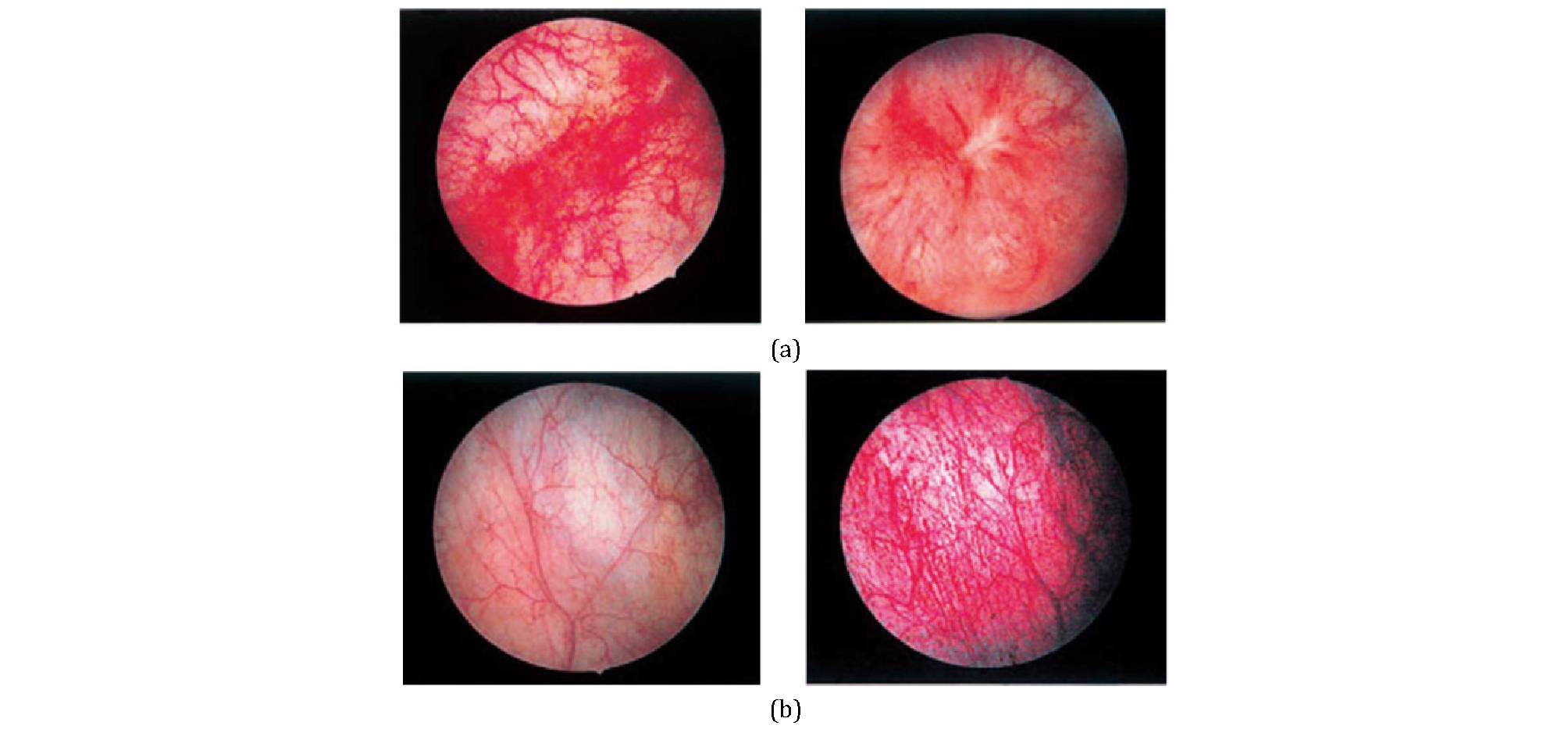
그림 1. (a) Hunner lesion. Hunner lesion is a reddish mucosal lesion lacking in the normal capillary structure associated with converging vessels, covering fibrinclots or scars in the vicinity. (b) Mucosal bleeding after distension. The apparently normal bladder (left) undergoes bleeding from the multiple sites during emptying after hydrodistension (right)
BPS/IC도 전립선비대증처럼 증상점수표로 환자의 증상을 먼저 확인하여 환자가 어느 정도의 통증을 가지고 있으며 불편한 가를 객관화 시키려는 노력이 있었다. 현재 BPS/IC의 증상 설문지는 University of Wisconsin IC Scale, O'Leary-Sant IC Symptom Index and IC Problem Index 그리고 Pelvic Pain and Urgency/ Frequency (PUF) Scale 등이 있으며 O'Leary-Sant symptom and problem index 가 주로 사용 된다 [8-10].
2.2. 치료
BPS/IC에 대한 치료법은 일반적으로 비특이적이며 경험적이라고 말할 수 있으며 증상의 개선을 목표로 한다고 하겠다. 일단 BPS/IC로 진단되면 다음 단계로 교육을 통해 질환에 대해 이해를 시키고 다양한 치료 방법, 즉 보존적, 약물적 또는 수술적 치료 등에 대한 정보는 제공함으로써 환자들로 하여금 자신의 치료 방향에 따른 조절과 선택이 많음을 인식하게 해야한다. 현재 BPS/IC의 치료는 행동요법에서부터 약물치료, 방광 내 약물주입요법, 수술적 치료에 이르기까지 다양하게 시도되고 있다. 최근 AUA에서는 BPS/IC 진단과 치료에 대해 6단계로 분류하였다 [11].
2.2.1. 1차 치료방법
BPS/IC 환자의 대다수는 특정 음식과 음료 섭취로 증상이 악화된다. 대부분은 산성음료, 커피, 매운 음식, 알코올음료 등이다. Interstitial Cystitis Association (https://www.ichelp.org)에서는 권고하는 음식과 피해야 할 음식들을 소개하고 있다. 골반저근운동과 방광훈련은 배뇨량의 증가와 빈뇨 증상의 완화에 도움이 되며, 배뇨일지는 환자와 임상의 모두에게 증상의 중증도를 객관적으로 측정할 수 있는 정보 및 방광 재교육의 기초를 제공한다. 심리적 스트레스 줄이기 등도 보존적 요법으로 이용될 수 있다.
2.2.2. 2차 치료방법
물리치료 (골반저 물리치료 또는 통증유발부위의 주사치료), 약물치료와 방광 내 주입요법이 포함된다.
약물 치료로는 Pentosan polysulfate sodium, Amitriptyline와 항히스타민제가 있다 [3], [표 3]. Pentosan polysulfate sodium는 헤파린과 비슷한 구조를 가지고 있으며 방광점막을 덮고 있는 점액다당류의 합성제제로써 투여 시 방광점막층을 보호하여 소변 내에 존재하는 독성 물질로부터 방광점막을 보호하는 작용을 한다. 삼환계항우울제인 amitriptyline은 중추 및 말초의 항콜린작용과 신경 말단부에서 세로토닌과 노르아드레날린의 재흡수를 억제하며, 중추에서 항히스타민작용에 의한 진정효과를 나타낸다. 취침 시에 25mg으로 투여하기 시작하여 점차 증가하여 100mg까지 증량시킨다. 항히스타민제는 간질성방광염에서 중요한 역할을 하는 것으로 생각되는 비만세포의 탈과립 (degranulation) 시 분비되는 히스타민 등의 통각물질을 억제함으로서 증상의 호전을 기대할 수 있다. 그러나 인체로의 흡수율이 낮아 치료효과는 미약한 편이다. 장기간의 적절한 통증치료는 간질성방광염과 같은 만성 통증성 질환에 매우 중요한 역할을 한다. 신경병증성 통증에 사용하는 항우울제, 항전간제, 마약성진통제 등을 사용 할 수 있으며, 아세토아미노펜, 아스피린 그리고 비스테로이드항염증제 등도 효과적이다. 최근에는 항전간제인 Gabapentin의 효과를 보고하기도 하였다.
표 3. Standard dosages for commonly used treatments for BPS/IC
aIf symptoms improve, taper should be stopped, or if side effects persistmore than a day or two, the patient should bemaintained on the lowest dose previously tolerated for up to 2 weeks to determine maximal benefit.
방광 내 주입요법은 방광 내에 고농도를 유지하면서 전신적 부작용을 줄일 수 있다. 그러나 도뇨관 삽입이 필요하며 그로 인한 통증과 감염의 위험이 있고 치료비 상승의 부정적인 면도 있다. Dimethyl sulfoxide (DMSO)는 하부요로의 구심성 통각 신경로의 탈민감, 항염증작용, 진통작용, 근이완작용 및 콜라겐 용해 등의 다양한 약리학적 기전을 가지고 있어 간질성방광염의 치료에 유용하다. DMSO는 1-2주 간격으로 4-8회 치료하며 방광 내 주입한 후 15-20분 뒤에 배뇨시키는 방법이 널리 사용되고 있다. Hyaluronic acid Hyaluronic acid는 비황산화 점액다당류로서 GAG의 성분으로 알려져 있으며 점막 하 결체조직에 풍부하게 존재 한다. 간질성방광염 환자에서 hyaluronic acid의 작용기전은 hyaluronate의 보충, 자유라디칼 제거, 면역반응조절 등이 알려져 있다.
2.2.3. 3차 치료방법
방광 수압확장술 (bladder hydrodistention)은 간질성방광염의 최초 치료로서 많이 사용하고 있으며, 수압을 이용하여 방광을 확장시키는 방법으로 일시적으로 증상이 호전될 수 있지만 영구적인 것은 아니며 반복시술이 필요할 수도 있다. 방광 수압확장술에 대한 정확한 가이드라인은 정해져 있지 않으며 한 연구에서는 [12]은 8분 동안 80cmH2O의 수압으로 방광확장을 시행하여 방광용적이 큰 군에서는 12%, 방광용적이 적은 군에서는 26%에서 효과가 있었다고 하였다. 그러나 6개월 이상 증상호전이 지속 되지는 않았다. 방광 내 궤양의 경요도 절제술이나 전기나 레이저소작 법으로 동통을 조절할 수 있다.
2.2.4. 4차 치료방법
BPS/IC 환자에서 보툴리누스독소의 배뇨근 주사치료는 다른 치료 이후에도 증상이 조절되지 않을 때 시행될 수 있으나 수술 후 배뇨곤란으로 인한 자가도뇨를 시행할 수 있다는 점을 환자들에게 미리 알려야 한다. 천수신경조절술도 시행할 수 있다. 천수신경조절술은 천수신경을 자극함으로써 불안정한 신경반사를 억제하고 정상적인 배뇨로 되돌릴 수 있다고 보고됨에 따라 절박뇨, 특발성 만성요폐 뿐만 아니라 골반통, 간질성방광염에서도 그 시행이 확대되고 있으나 아직 BPS/IC의 치료에 대해서는 FDA에서 승인되지 않았다.
2.2.5. 5차 치료방법
Cyclosporine A가 소개되었으며 면역억제제로서 T-세포의 활동과 cytokine의 분비를 억제한다.
2.2.6. 6차 치료방법
수술적 치료는 보존적 치료가 실패한 경우에 고려해 볼 수 있다. 간질성방광염의 수술적 치료에서 부분방광절제술, 방광성형술 (cystoplasty), 방광삼각부 상부 또는 하부 방광절제술 (supratrigonal or subtrigonal cystectomy), 방광절제술 및 비실금형 (cystectomy with continent pouch) 요로전환술 등이 포함된다.
3. 결 론
현재 BPS/IC에 대해서 확실한 것은 거의 없으며, 진단에 있어서도 방광 불편감 혹은 통증, 빈뇨 등을 일으킬 수 있는 다른 모든 원인질환을 배제하는 것이 중요하다. 정밀검사로 배뇨일지, 현미경적 요검사 및 요배양검사, 방광경검사가 포함된다. 적응증이 된다면 요 세포검사, 요역동학검사, 방사선학적 검사, 방광 조직검사 혹은 복강경 검사 또한 요구될 수 있다. 새로운 간질성방 광염 진단 표식자에 대한 연구가 많이 이루어지고 있으나 아직 명확한 연구 결과는 없으며, 증상설문지는 예후를 추적하는데 도움이 될 수 있다. 치료는 질환을 이해하는 것부터 보존적치료, 경구제 투여, 방광 내 약물투여 그리고 수술적 치료 등이 있다.
