
1. 서론
2. 본론
2.1. 충분한 약물 복용 시도(Sufficient medication attempts)
2.2. 약물 용량 증대(Increased PDE5I dose)
2.3. 다른 용법으로의 교체(Change to different dosing regimen)
2.4. 다른 약제로의 교체(Change to different drugs)
2.5. 매일 복용법과 필요시 복용법의 복합치료(Combined long- and short-acting drugs)
2.6. 일부 항우울제의 추가(Addition of some anti-depressants)
2.7. 정신과적 치료의 추가(Addition of psychosexual therapy)
2.8. 적극적인 파트너의 역할(Role of the sexual partner)
2.9. 발기와 관련된 기저 질환 및 약물(Comorbidities and medications)
2.10. 테스토스테론의 추가(Addition of testosterone)
2.11. 생활습관 교정(Lifestyle modification)
3. 결론
1. 서론
1998년 비아그라(성분명: sildenafil)가 시장에 첫선을 보인 이후로, phosphodiesterase-5- inhibitor (PDE5I)는 발기부전 치료의 가장 기본이 되는 약물이면서 동시에 가장 많이 시행되는 치료 방법이다. 국제성의학회나 유럽비뇨의학회를 비롯한 많은 전문학회들의 진료지침에서도, PDE5I는 원인과 관계없이 발기부전의 일차치료로 추천된다.
그럼에도 불구하고, PDE5I를 복용한 환자들의 약 30-35%는 효과가 없거나 부족하다고 느낀다 [1]. 이러한 통계는 일반적인 기대보다 훨씬 높은 것으로, 환자 진료시에 어려움을 야기할 수 있다. PDE5I가 효과가 없거나 부족한 경우, 음경해면체내 주사요법이나 음경보형물 삽입술 등이 다음 단계 치료법으로 고려된다. 하지만, 이러한 방법들은 PDE5I에 비하여 상대적으로 침습적이며 환자교육이 더 어렵다. 따라서, 이러한 다음 단계의 치료 방법들을 고려한다면, 그 적절성에 대하여 신중한 판단 및 적절한 환자 상담이 반드시 필요하다.
PDE5I가 효과가 없거나 부족한 이유는 크게 2가지로 나눈다. 첫째, 약물 복용방법이 부적절한 경우(incorrect drug use)로, 환자의 약물 복용 방법을 다시 한 번 점검하여야 한다. 둘째, 약물 자체의 효과가 부족한 경우(lack of efficacy)로, 약물 효과를 감소시킬 수 있는 원인이나 약물 효과를 증대시킬 수 있는 방법에 대하여 다시 한 번 고려하여야 한다.
본 글에서는, 문헌들에서 소개되는 증거들을 바탕으로, PDE5I가 효과가 없거나 부족한 경우에 다음 단계 치료로 넘어가기 전에 의료진이 고려하여야 하는 문제들 및 해결을 위해 시도해볼 수 있는 방법들에 대하여 소개하고자 한다.
2. 본론
2.1. 충분한 약물 복용 시도(Sufficient medication attempts)
가장 먼저 고려해 볼 것은, 충분한 시도를 해보았는가 하는 것이다. 여러 연구들에서, PDE5I의 종류나 용량에 관계없이 시도를 많이 할수록 그 성공율은 증가한다 [2,3,4]. 일반적으로 적어도 6회 이상의 시도를 해볼 것을 권고하고 있으며, 이 경우 80% 이상의 성공율이 보고된다.
2.2. 약물 용량 증대(Increased PDE5I dose)
약물 용량을 증대시키는 것이 하나의 방법이 될 수 있다. 용량 증대에 정비례하지는 않지만, 대략 10-50% 정도의 추가적인 발기능의 향상을 기대할 수 있다 [5,6,7]. 따라서, 약물과 관련된 위험도나 부작용 가능성이 크지 않다면, 허가 범위내에서는 고용량부터 시도해 보는 것이 좋을 수도 있다.
2.3. 다른 용법으로의 교체(Change to different dosing regimen)
Tadalafil과 udenafil의 저용량 매일 복용법(daily dosing regimen)은 잘 알려진 치료 방법이다. 이러한 약제들에서, 필요시 복용법(on demand dosing regimen)이 효과가 없거나 부족한 경우에 매일 복용법은 상대적으로 저용량임에도 불구하고 발기능 향상에 도움이 될 수 있다 [8]. 흥미로운 것은, 상대적으로 반감기가 짧아 매일 복용법에 대하여 허가받지 않은 약제들도 유사한 효과를 보인다는 것이다 [9]. 즉, 필요시 복용법과 매일 복용법은 어느 한가지 방법이 효과가 없는 경우 다른 방법으로 교체해 보는 것이 도움이 될 수 있다.
2.4. 다른 약제로의 교체(Change to different drugs)
여러 다양한 PDE5I들은 PDE5 선택성, 작용시간, 반감기 등이 각기 다르며, 이에 대한 반응도 환자 개개인에 따라서 다르게 나타날 수 있다 [표 1]. 따라서, 비록 넓은 의미에서는 같은 PDE5I라 하더라도 다른 약제로의 변경이 발기능 향상에 도움이 될 수 있다.
표 1.
PDE5I의 약동학
| sildenafil | vardenafil | tadalafil | udenafil | mirodenafil | avanafil | |
| 최고농도 도달시간 | 1.0 | 0.8 | 2 | 1.4 | 1.3 | 0.5 |
| 작용 시간 | 4-5 | 4-5 | 36 | 12 | 4-6 | 7-10 |
| 반감기 | 4 | 4-5 | 17.5 | 10 | 2.5 | 1.5 |
2.5. 매일 복용법과 필요시 복용법의 복합치료(Combined long- and short-acting drugs)
저용량의 매일 복용법은 음경재활(penile rehabilitation)을 목적으로 하며, 고용량의 필요시 복용법은 즉각적인 발기(immediate effect)를 목적으로 한다. 각 용법의 약리 생리학적 기대효과가 다르기 때문에, 복합요법은 추가적인 발기능 증대를 기대할 수 있으며, 동시에 부작용은 감수할만한 정도였다 [10,11].
2.6. 일부 항우울제의 추가(Addition of some anti-depressants)
트라조돈(trazodone)은 흔히 처방되는 항우울제 중의 하나로, 중추신경계에서 세로토닌 재흡수를 억제하고 음경에서는 알파 아드레날린 수용체의 작용을 억제하여 발기능 향상에 도움이 되는 것으로 알려져 있다 [12]. 아울러 우울 증상의 호전 역시 발기능에 도움이 될 수 있다. 따라서, 트라조돈을 포함한 일부 항우울제들은 PDE5I에 반응하지 않는 환자들에서 추가적인 발기능 향상을 기대할 수 있다.
2.7. 정신과적 치료의 추가(Addition of psychosexual therapy)
비뇨의학 전문의가 접근하기 쉽지 않은 치료방법이기는 하지만, 정신치료, 행동치료, 인지치료, 최면치료, 마음 챙김 요법, 집단 치료 등 정신과적 치료가 도움이 될 수 있다. 흥미로운 것은, 일부 연구에서 정신과적 치료의 기간, 치료 방법의 종류, 의료진의 숙련도가 증상 호전에 큰 영향을 주지 않는 것으로 보고하였다 [13]. 즉, 부족한 정신과적 접근이라 하더라도 아예 안하는 것보다는 작은 지지요법(supportive care)이라도 시행하는 것이 도움이 된다.
2.8. 적극적인 파트너의 역할(Role of the sexual partner)
국내 현실에서, 파트너를 같이 상담하는 것이 흔하지는 않다. 하지만, 파트너와의 상담은, 환자의 불안과 스트레스 감소, 성적 친밀도의 호전, 성적 활동의 변화 및 생활 습관의 교정 등 발기능 향상에 도움이 된다 [14,15].
2.9. 발기와 관련된 기저 질환 및 약물(Comorbidities and medications)
당뇨나 고혈압, 고지혈증 등의 기저 질환들과, 항암제, 항안드로겐제, 베타차단제 등의 일부 혈압약, 정신신경계통 약물 등은 발기부전의 원인이 되거나 발기부전을 악화시킬 수 있다 [표 2]. 아울러, 이러한 요인들은 발기부전 치료를 더 어렵게 만들며, PDE5I의 효과를 감소시키는 요소로 작용하게 된다 [16]. 따라서, 이러한 위험 요인들을 파악하고, 할 수 있다면 피할 수 있는 방법을 찾아보는 것이 중요하다.
표 2.
발기부전과 연관된 질환 및 약물
2.10. 테스토스테론의 추가(Addition of testosterone)
발기부전 및 그 치료에서 남성호르몬은 빼놓을 수 없는 요소이다. 이론적으로, 남성호르몬은 PDE5I의 반응을 증가시키며, PDE5I는 남성호르몬의 분비를 자극한다 [17]. 하지만, 여러 메타분석 결과들에서는, PDE5I 단독 치료에 비하여 테스토스테론 복합치료가 발기능의 향상에 더 도움이 되기는 하지만, 그 효과가 일반적인 기대만큼 크지는 않았다 [18,19,20].
여러 연구 결과들과 진료지침들을 종합해보면, 테스토스테론 복합치료는 PDE5I에 효과가 없거나 부족한 경우에 시도해 볼 수 있는 옵션임은 분명하다. 다만, 주의하여야 할 점은 남성갱년기가 있는 경우에 해당된다는 것이며, 남성갱년기가 없는 경우에는 아직 권고되지 않는다는 것이다 [21].
2.11. 생활습관 교정(Lifestyle modification)
가장 기본이지만 흔히 놓치기 쉬운 것이 생활습관 교정이다. 꾸준한 운동과 비만 교정, 건강한 식단, 과도한 음주 자제, 금연 등은 발기부전 치료에 도움이 될 뿐만 아니라, 환자와의 신뢰도 형성에도 도움이 된다 [표 3]. 생활습관 교정은 꾸준한 관리가 중요하며 적절한 효과를 가지려면 적어도 3-6개월 이상의 관리가 필요하다 [22].
표 3.
발기부전의 예방/치료에 도움이 되는 생활습관
3. 결론
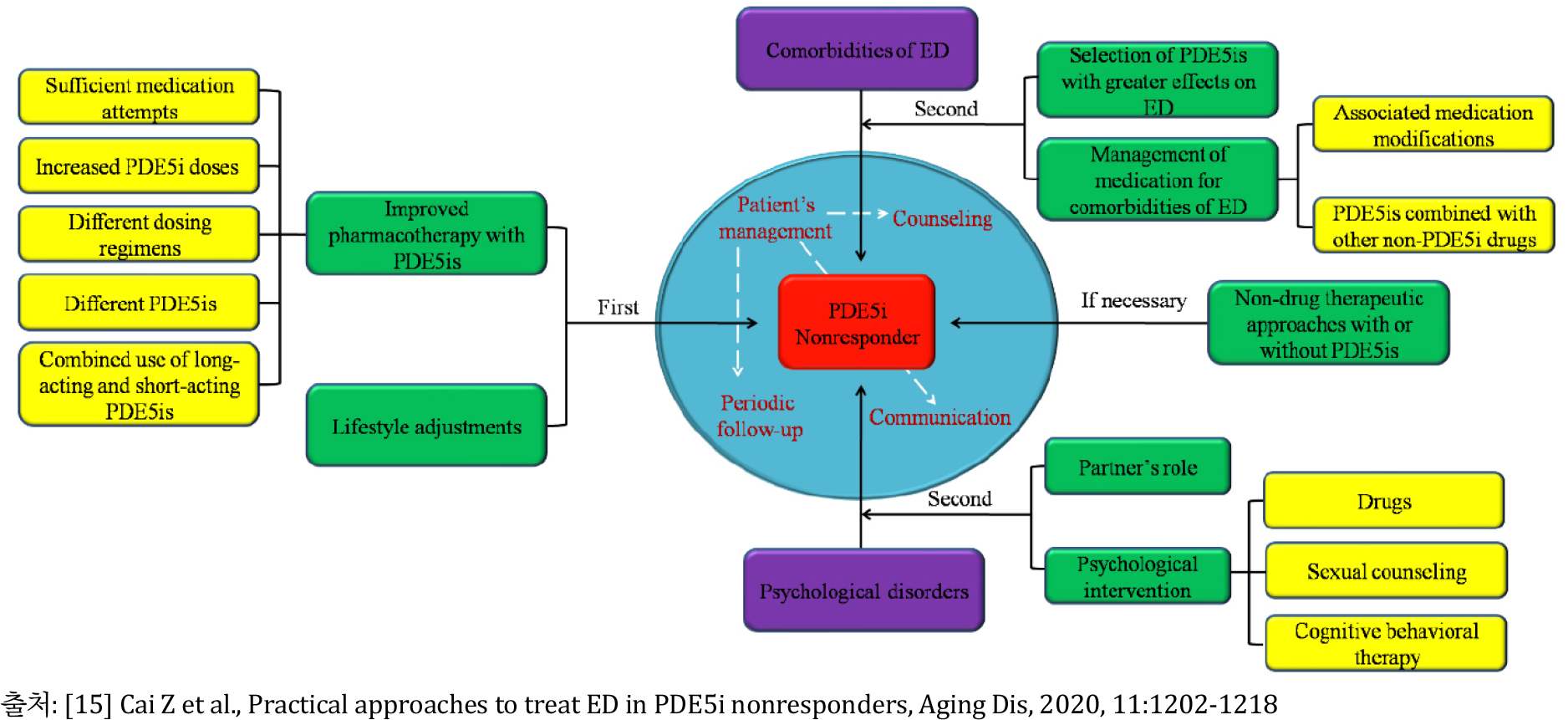
요약하자면, PDE5I가 효과가 없거나 부족한 경우, PDE5I가 제대로 사용되고 있는지 그 효과를 올릴 방법이 없는지를 먼저 고려하여야 한다 [그림 1]. 교정할 수 있는 동반질환이나 약물에 대해서도 고려하여야 하며, 생활습관 교정도 권고하여야 한다. 아울러 환자의 정신심리적 상태에 대해서도 충분히 고려하여야 한다.
상기의 과정을 거친 후에도 발기부전의 호전이 만족스럽지 못하다면, 이차 혹은 삼차 요법에 대해서 환자와 충분한 상의를 하여야 한다.
