1. 항혈소판제
1.1. 1차 예방 치료를 받는 경우 항혈소판제의 복용관리
1.2. 2차 예방 치료를 받는 경우 항혈소판제의 복용관리
2. 항응고제
2.1. 항응고제의 종류
2.2. 시술에 따른 출혈 위험도
2.3. 환자에 따른 혈전생성위험도
3. 결론
1. 항혈소판제
Aspirin은 혈소판의 cyclooxygenase를 비가역적으로 억제하여, 혈소판에서 강력한 혈소판 응집 인자인 thromboxane A2의 생성을 막아 항혈소판 작용을 나타낸다. 시술 전후 가장 적절한 항혈소판제 복용의 관리는 아직까 지 명확하게 밝혀지지 않았으나 2012 American College of Chest Physicians (ACCP) 지침에서는 모든 시술 7일 전부터 항혈소판제 복용을 무조건 중단하는 것은 과장된 방법이라고 밝힌다 [1]. 시술 전후 항혈소판제 복용 관리를 위해서는 언제나 각 시술이 지닌 출혈의 위험도와 항혈소판제 복용 중단으로 인한 혈전 생성의 위험도를 동시에 고려해주어야 한다. 항혈소판치료는 크게 1차 예방 치료(primary prevention therapy)와 2차 예방 치료(secondary prevention therapy)로 나뉜다. 1차 예방 치료는 50세 이상의 성인이 심뇌혈관질환 발생 예방을 위하여, 또는 관상동맥 스텐트를 삽입한 지 1년이 지나거나 심뇌혈관질환이 발생한 지 1년이 지나 안정적인 단계에 있는 환자가 재발 방지를 위해 아스피린을 지속적으로 복용하는 것을 말한다 [2]. 2차 예방 치료는 최근 심뇌혈관질환이 발생하였거나 스텐트를 삽입한 후 1년이 지나지 않은 환자가 스텐트 내 혈전 발생 예방을 위해 항혈소판치료를 받는 경우를 말한다.
1.1. 1차 예방 치료를 받는 경우 항혈소판제의 복용관리
1차 예방 목적으로 아스피린을 복용 중인 환자가 백내장 수술, 피부과적 시술, 치과적 시술, 그리고 점막 생검 등을 포함한 내시경적 시술과 같은 저출혈성 위험도를 가진 시술을 받기 전에는 아스피린 복용을 중단하지 않아도 된다 [3], [4], [5], [6]. 반면, 두개 내 수술이나 경요도적 전립선절제술 같은 출혈성 위험이 큰 수술에 경우에는 아스피린을 중단하는 것이 좋다. 그 외의 중증도의 출혈성 위험이 있는 시술을 위해서 아스피린 복용을 지속할지 중단할 지의 여부는 시술 자의 재량에 맡긴다. 일반적으로, 관상동맥 스텐트를 삽입하지 않고 있으며 최근 3개월 동안 심뇌혈관질환의 발생의 과거력이 없어 심뇌혈관 합병증 발생 위험도가 낮은 환자에서는 시술 7-10일 전 아스피린을 중단하는 것을 권장한다. 심혈관 합병증 발생 위험도가 중증도 이상이면서, 비심장적 수술을 받는 경우에는 아스피린 복용을 지속하는 것이 권장된다 [1]. 혈소판의 수명이 평균 10일 정도라는 것을 감안하면 아스피린을 복용하던 환자가 약 7일간 중지하면 혈액 응고를 억제하는 효과는 거의 없어지게 된다. 그리고 3일 이상 중지하면 중대한 혈액 응고 저하의 위험성은 거의 없어진다. 그러므로 발치 등과 같은 간단한 수술을 위해서는 아스피린을 3일에서 5일간 중단하는 것이 바람직하며 큰 수술을 위해서는 약 7일간만 중단하는 것이 추천되며 목적한 수술이 끝난 후에는 지혈의 정도를 봐서 당일 혹은 그 다음 날 다시 시작하도록 한다.
1.2. 2차 예방 치료를 받는 경우 항혈소판제의 복용관리
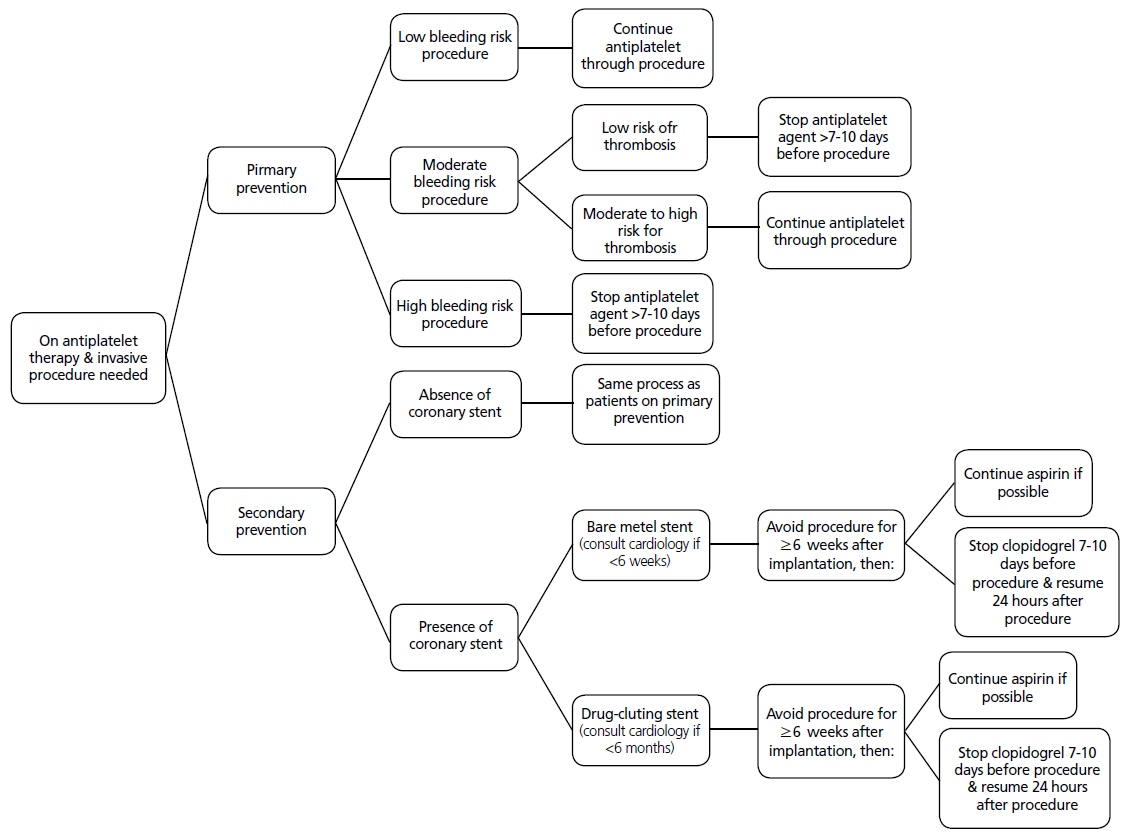
2차 예방 치료를 받는 환자에서도 저출혈성 위험도의 수술 또는 시술을 받는 경우는 1차예방 치료를 받는 환자에서와 마찬가지로 항혈소판제 치료를 지속하는 것을 추천한다. 그 외의 시술에서는 출혈의 위험성과 혈전 생성의 위험도를 판단하여 치료 지속 여부를 결정한다 [1]. 그러나 관상동맥 스텐트 삽입술을 한 환자의 가장 중요한 합병증은 스텐트 안에 생성되는 혈전의 재생성으로, 64%의 환자에서 심근경색이 발생하거나 사망에 이르게 할 수 있다 [7]. 스텐트 내 혈전 발생은 아스피린과 클로피도그렐의 복합치료로 감소시킬 수 있다 [2]. 최소 4-6주에서 최대 12개월까지 항혈소판제 복합치료하는 것을 권장하고 있다 [1,8]. 스텐트의 종류는 재질에 따라 크게 맨금속 스텐트(bare metal stent)와 약물방출 스텐트(drug-eluting stent)로 나누는데, 맨금속 스텐트 삽입 6주, 약물방출 스텐트 삽입 6개월 이내에 수술적 시술을 받는 경우는 아스피린과 클로피도그렐 복용을 지속하는 것을 권장한다 [1,7]. 만약 출혈 위험성이 크다면, 심장전문의와 상담하여 치료 지속 여부를 결정해야한다. 약물방출 스텐트를 삽입한 환자가 클로피도그렐을 중단해야 하는 시술을 받을 경우, 가능하다면 아스피린은 지속적으로 복용해야 한다. 그리고 시술이 끝난 후에는 클로피도그렐을 되도록 빨리 복용하는 것이 좋다.
만약 출혈로 인한 위험도가 스텐트 내 혈전 생성 위험도보다 크다면 시술 전 항혈소판제 치료를 중단하고, 시술 후 최대한 빨리 항혈소판제 복용을 재개하는 방법이 추천된다. 위와 같은 권장 지침사항을 [그림 1]에 정리해보았다 [1,8].
2. 항응고제
대표적인 항응고제인 와파린과 같은 비타민 K 길항제는 심방세동(atrial fibrillation), 심부정맥혈전증(deep vein thrombosis)을 가진 환자, 인조 심장 판막(artificial heart valve) 수술을 시행한 환자의 혈색전증(thromboembolism) 발생을 예방하기 위해 처방한다. 또한 이런 환자들 시술 혹은 수술을 받게 될 경우 역시 출혈의 위험성과 혈색전증 발생의 위험성을 고려하여 시술 전, 후 항응고제 복용 관리를 하여야 한다.
2.1. 항응고제의 종류
2.1.1. 와파린
간에서 만들어지는 응고 인자인 factor II, VII, IX, X과 항응고 물질인 Proetin C, S 등은 생성/활성화 과정에 비타민 K가 필요한데 Warfarin은 이러한 비타민 K의 작용을 차단하여 혈액 응고 인자의 활성화를 억제하게 된다.
와파린 투여시에는 혈액 응고 인자는 물론 항응고 인자의 혈장내 농도도 같이 감소하게 되는데 특히 투여 초기에는 반감기가 짧은 Protein C의 농도가 먼저 감소하게 되어 오히려 혈전 형성이 유발될 수 있어 투여 초기에는 Heparin과 동반 투여하다 항응고 효과가 목표 범위에 이른 후 Heparin을 중지하여야 한다.
항응고 효과는 표준화된 Prothrombin time인 INR (International Normalized Ratio)를 이용하여 INR이 2.0~3.5 범위를 유지하도록 한다.
2.1.2. Direct thrombin inhibitor
최근에는 Direct thrombin inhibitor는 thrombin에 직접 부착되어 작용을 차단한다. Heparin에 비하여 이미 fibrin과 결합하였거나 액체 상태의 thrombin의 작용도 차단할 수 있다는 장점이 있으나 antidote가 없다는 것이 중요한 단점이다. 현재 FDA에서 사용이 허가된 Direct thrombin inhibitor에는 hirudin, argatroban, bivalirudin 등이 있는데, hirudin은 heparin-induced thrombocytopenia (HIT) 환자에서 heparin의 대체 용도로, argatroban은 HIT에서의 heparin 대체와 HIT의 위험성이 높은 환자의 관동맥 중재술시, bivalirudin은 관동맥 중재술을 시행하는 환자에서 heparin의 대용으로 사용하고 있다.
2.1.3. Factor Xa inhibitor
Factor Xa inhibitor에는 factor Xa에 직접적으로 결합하여 작용을 억제하는 direct inhibitor와 factor Xa에 대한 antithrombin의 작용을 증강시키는 indirect inhibitor가 있다. Indirect factor Xa inhibitor에 대표적인 약제는 fondaparinux로 피하 투여로 흡수율이 높으며 혈중 반감기가 17시간으로 1일 1회 투여가 가능하며, heparin과 같은 heparin induced thrombocytopenia 위험성이 없다는 장점이 있다. 현재 급성 관상동맥증후군, 정맥 혈전증 환자 대상의 임상연구가 진행되고 있다. Direct factor Xa inhibitor는 indirect inhibitor에 비하여 유리된 형태의 활성 factor Xa는 물론 이미 혈소판과 결합된 factor Xa의 작용도 차단할 수 있다는 우월성을 지닌다. 경구 복용이 가능하다는 점이 또 하나의 중요한 장점인데 가장 먼저 개발된 약제는 Rivaroxaban으로 정맥 혈전증 예방, 심방세동 환자에서의 뇌졸중/혈전 합병증 방어에 대한 3상 연구가 진행 중이다. 그 외 Apixaban 을 비롯한 여러 약제가 개발되고 있다.
2.2. 시술에 따른 출혈 위험도
몇몇 시술들은 출혈성 위험도가 매우 낮아 항응고제 복용을 중단하지 않고 시행하여도 안전하다. 이러한 경우, 항 응고제 복용을 중단하고 교락 치료(bridging therapy)를 시 작함으로써 발생하는 위험성과 비용이 감소한다.
2.2.1. 저출혈성 위험도의 시술: 항응고제 복용을 지속
2.2.2. 고출혈성 위험도의 시술: 항응고제 복용 중단 필요.
| 요추 천자(lumbar puncture)와 심도자술(cardiac catheterization)의 경우는 출혈성 경향이 있어 항응고제를 중단하는 것을 권고한다[13], [14], [15]. 용종절제술(polypectomy), 담관 괄약근절제술(biliary sphingectomy), 정맥류 치료술(variceal treatment), 경피적 내시경적 위절개 삽입술(percutaneous endoscopic gastrotomy placement), 협착 확장술(dilation of strictures), 초음파를 이용한 내시경적 미세바늘흡인검사(endoscopic ultrasound-guided fine needle aspiration) |
2.3. 환자에 따른 혈전생성위험도
항응고제 복용 중인 환자에서 언제, 어떻게 시술 전후 헤파린 교락치료(bridging therapy)를 하는 경우는 혈전생성위험도에 따라 다르다. 혈전 생성의 위험도가 낮은 경우는 헤파린 교락치료가 필요하지 않고, 높은 경우는 헤파린 교락치료가 필요하다 [1], [17], [18], [19], [20], [21], [22].
2.3.1. 혈전생성도 위험도가 낮은 경우
2.3.2. 혈전생성도 위험도가 높은 경우
|
⦁주요 흉부 수술, 두개내 혹은 척추 수술, 주요 혈관 수술, 주요 정형외과 수술, 방광 혹은 전립선에 관련된 비뇨기과 수술, 주요 종양 수술, 성형외과적 재건술, 용종제거를 하는 결장경, 신장 혹은 전립선 생검술, 심박조율기, 심제세동기 삽입술(cardiac pacemaker/defibrillator placement) ⦁시술 전 관리 시술 24시간 전에 마지막 헤파린을 투여하고, 만약 전 용량의 저 분자 헤파린(a full once-daily dose)을 투여하는 경우에는 시술 시 잔여 항응고작용을 제거하기 위해 수술 전날에는 용량을 반으로 줄여 투여해야 한다고 권장하고 있다 [1]. ⦁시술 후 관리 수술 후 헤파린 치료의 재개는 출혈 위험성 정도가 높은 시술의 경우 시술 후 48시간 이후에 한다. 항응고치료 재개 시 지혈 정도와 출혈 정도를 증가시키는 환자 자체 요인으로는 고령, 항혈소판제 혹은 비스테로이드 성소염제 동반 복용, 신기능 부전, 척추, 경막외 카테터 삽입, 간질환 악화, 악성 종양과 같은 동반 질환의 여부 등이 있다 [27]. ACCP는 수술 후 출혈 위험성이 높다고 생각되는 환자에서는 수술 후 48-72시간까지 전용량 항응고치료(full- dose anticoagulation)를 보류하는 것을 추천하고 있다. |