
1. 서론
2. 본론
2.1. 인지기능 장애를 평가할 수 있는 간단한 선별검사 도구: MMSE (Mini-Mental State Examination, 간이정신상태검사)
2.2. Anticholinergic Burden을 측정하는 방법: Korean version anticholinergic burden scale (KABS)
2.3. KABS 적용 임상 연구와 항콜린약물부담에서 비뇨의학과 약물의 기여도
2.4. 고령에서 항콜린제의 사용시 고려사항과 대체약물
3. 결론
1. 서론
고령의 환자에서 하부요로증상으로 항콜린제를 쓰는 경우가 많아지고 항콜린제가 인지기능을 악화시키거나 치매를 유발하는 위험인자라는 연구가 보고되며 인지기능을 평가하여 항콜린제 사용을 중단하거나 적절한 다른 약물로 대체를 할 필요성이 생겼다 [1].
이러한 과정을 실행하기 위해서는 다음 두 가지 문제가 해결이 되어야 한다. 첫째는 항콜린제 사용 전 후를 비교하기 위해 인지기능을 비교적 간단히 평가하고 반복적으로 사용을 할 수 있는 도구가 있어야 한다. 둘째는 항콜린효과를 갖는 약물은 매우 다양하며 광범위하게 사용되고 있어서 체계적인 분류 및 효과의 강도를 알 수 있어야 하고 실제 임상에서 환자가 사용 중인 약물들이 항콜린효과가 있는 지를 쉽게 평가하고 효과 크기를 알 수 있는 도구가 있어야 한다. 두 가지 도구를 이용하여 실제 임상에서 고령 환자의 인지기능을 평가하고 항콜린제 약물의 사용을 적절히 조절한다면 안전한 진료를 할 수 있다.
2. 본론
2.1. 인지기능 장애를 평가할 수 있는 간단한 선별검사 도구: MMSE (Mini-Mental State Examination, 간이정신상태검사)
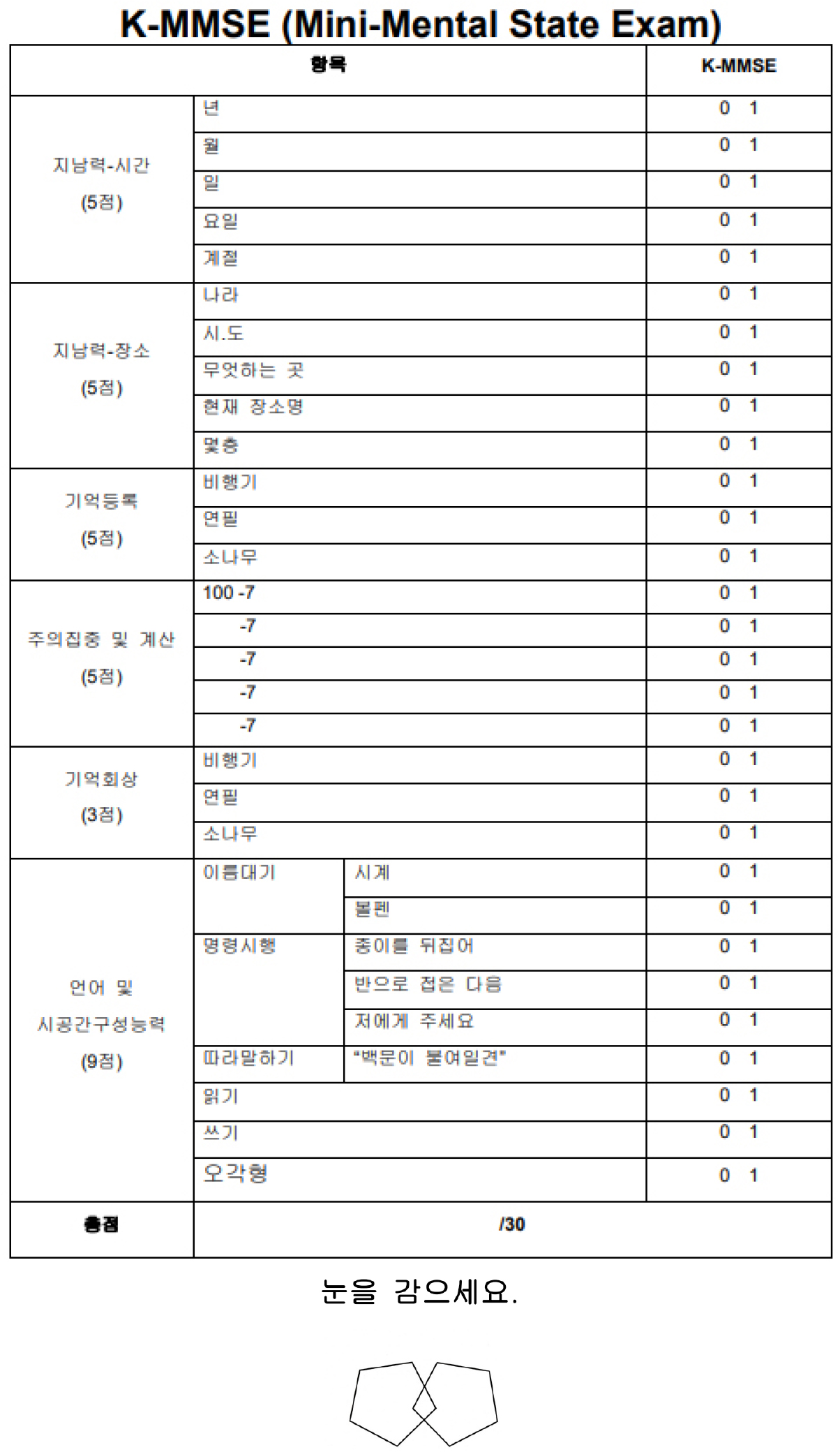
외래에서 인지기능저하가 의심되는 경우 짧은 시간에 간단히 인지기능을 평가하는 도구는 신경과나 정신과에서 널리 사용하고 있다. 실제 임상에서 인지기능평가를 위해 널리 사용되는 선별검사로 MMSE (Mini-Mental State Examination, 간이정신상태검사)가 있다 [2]. 적절한 훈련을 받은 검사자가 간단한 준비물(펜, 시계, 지우개, 빈 종이)로 5-10분 정도 짧은 시간에 질문하면서 채점하는 방법으로 시행할 수 있고, 반복검사로 인한 연습효과가 적어 반복측정이 용이하며 항콜린제 사용에 따른 인지기능의 변화를 측정할 수 있다. 약물의 사용 전 후 변화를 확인하면서 점수 저하가 뚜렷하면 약물 중단이나 대체를 고려하는 기준으로 삼을 수 있으며 신경과나 정신과 진료를 권유하여 조기 치매 발견에 도움이 될 수 있다.
MMSE는 19문항으로 이루어져 있고 치매에 대한 민감도는 0.86~0.92, 특이도는 0.92~0.99이다. 시간과 장소 5점, 지남력 5점, 주의력 5점, 기억등록 3점, 기억회상 3점. 구성능력 1점이며 총30점 만점이다. 24점 이상은 확정적 정상, 20~23점은 치매의심, 19점 이하는 확정적 치매로 평가하며 국내 번역본으로 K-MMSE [그림 1]가 있다. 또 다른 MMSE-K에서는 무학, 문맹의 경우는 시행점수 +4점(시간 지남력 +1점, 주의 집중력 +2점, 언어기능 +1점)을 추가하여 평가한다. 고학력자나 과거 기억력이 좋았던 대상자는 정상 범주에 있더라도 치매가 시작되었을 수 있으므로 평가에 주의를 요한다. 이러한 이유로 경도인지장애를 선별하는 데는 한계가 있다 [3]. 여러 버전의 MMSE가 표준화되어 사용 중인데, Korean version of MMSE (MMSE-K) [4], Korean MMSE (K-MMSE) [5], MMSE in the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) assessment battery (MMSE-KC) [6] 그리고 Korean version of MMSE for Dementia Screening (MMSE-DS) [7]가 있다. 이 중 K-MMSE의 실제 질문 방법에 대한 동영상(https://youtu.be/SJkSmFyX_Cs)을 참고해도 좋겠다.
다른 검사 도구는 몬트리올 인지평가(The Montreal Cognitive Assessment, MoCA)가 있다 [8]. 경도 인지장애에 조금 더 민감한 검사이나 15분 정도 소요되어 실제 바쁜 임상에서 활용되기에는 불편한 면이 있다. 국내에서는 표준화된 K-MoCA를 사용할 수 있다 [9].
2.2. Anticholinergic Burden을 측정하는 방법: Korean version anticholinergic burden scale (KABS)
노년기 두 가지 이상의 질환으로 인하여 여러가지 약물을 복용하는 경우는 일상적이다. 질병다발성(multiple pathology)로 인한 다약물복용(polypharmacy)이 발생하게 되고 이러한 약물들이 누적되어 또 다른 부정적인 영향을 만들 수 있다.
항콜린약물부담(anticholinergic burden)이란 같은 시기에 복용하는 항콜린성 약물의 누적 효과를 말한다. 항콜린성 약물을 평가하고 수치화하여 Anticholinergic Burden을 측정하는 방법들이 개발되어 사용되고 있다. 가장 많이 사용되는 방법들로 Anticholinergic Cognitive Burden Scale (ACB), Anticholinergic Drug Scale (ADS) 그리고 Anticholinergic Risk Scale (ARS) 등이 있으며, 국내에 유통되는 약물을 대상으로 Korean version anticholinergic burden scale (KABS)가 델파이 방법을 이용하여 개발되어 사용하고 있다 [10]. 총 494 종의 약물을 분류하여 0점부터 3점까지 항콜린효과의 강도를 구분하였다. 그 중 2점은 23 종, 3점은 56 종의 약물이 있으며 과민성방광에 사용 중인 항콜린제(Imidafenacin, Fesoterodine, Oxybutynin, Propiverine, Solifenacin, Tolterodine, Trospium)은 모두 3점으로 분류가 되었다. 실제 임상 진료에서 노인 환자가 복용하는 약물을 알고 목록에 있는 약제와 비교하여 점수의 합을 계산하면 항콜린약물부담의 크기를 알 수 있게 된다 [표 1].
표 1.
Medication lists and anticholinergic score (1-3) included in the Korean Anticholinergic Burden Scale
Modified from Ref. [10] Jun K et al. Geriatr Gerontol Int. 2019
2.3. KABS 적용 임상 연구와 항콜린약물부담에서 비뇨의학과 약물의 기여도
실제 국내 병원에서 KABS를 적용한 연구를 보면 어떠한 약물들이 가장 흔하게 문제가 되고 있으며 비뇨의학과에서 주로 사용하는 과민성방광 약물인 항콜린제는 어느 정도 영향을 주는 지 가늠해 볼 수 있다. 분당서울대학교병원 노인의료다학제팀(의사, 약사, 간호사, 영양사 및 사회복지사)에서 노인의료센터 입원환자(2018년 7월 1일부터 2019년 6월 30일 395명, 평균 연령은 82.7±8.7세)의 항콜린약물부담 감소효과를 분석한 연구 결과를 보면 KABS (Korean Anticholinergic Burden Scale) 목록의 항콜린성 약물을 1종 이상 복용 환자는 75.6%, 3점 이상 고노출군은 41.5%였다. 항콜린약물부담 기여도는 항정신병약제(23.1%), 항히스타민제(16.5%), 항우울제(10.8%), 수면진정제(10.5%)로 나타났고 개별 약물은 Quetiapine(디벤조티아제핀 계열에 속하는 조현병 치료제, 19.5%, 2점), chlorpheniramine (9.5%, 3점), tramadol (7.8%, 2점), furosemide (6.6%, 1점), escitalopram (4.8%, 1점), clonazepam (4.8%, 1점) 순이었다. 위험도는 10종 이상의 다약제를 복용하는 경우(3.7배), 요양시설 거주인 경우(2.85배) 증가하였다. 비뇨의학과 관련 약제는 5%미만의 기여도로 매우 낮게 나타났다 [11].
국내 건강보험 노인 코호트 데이터(2002년부터 2013년)를 이용한 빅데이터 연구에서 치매 진단을 받은 군(28,864명)과 치매 진단을 받지 않은 대조군(57,712명)을 대상으로 진단을 받기 전 9년간 사용된 항콜린약물의 양과 치매 유병률의 차이를 KABS와 Anticholinergic Cognitive Burden Scale (ACB)를 이용하여 분석하였다. 항콜린제 고노출군은 치매진단군에서 3.2%로 대조군 2.1%에 비해 높게 나타났다. 치매진단군에서 항콜린제 고노출인 경우 1.71배 위험도를 보여 저노출인 경우 1.22배에 비해 높았다. [표 2]에서 가장 많이 사용된 항콜린효과 약물은 chlorpheniramine (98%, 3점), tramadol (95.3%, 2점), cimetidine (95.2%, 2점) 순이었고 기여도는 cimetidine (11.6%), dimenhydrinate (11.3%, 1세대 항히스타민제, 멀미약)이 높았으나 비뇨의학과 약물인 Propiverine, Solifenacin, Tolterodine은 모두 2% 정도로 낮았다 [12].
표 2.
Top 20 medications that contributed to the anticholinergic burden score in dementia patients with high exposure prior to2–10 years of dementia according to the scales
 |
Adapted from Ref. [12]Suh et al. BMC Geriatrics (2020).
두 연구 모두 비뇨의학과 관련 항콜린제는 항콜린효과 점수가 3점으로 가장 높지만 기여도는 낮게 나타났다. 이는 실제 임상에서 항콜린효과를 강하게 갖고 기여도가 높은 약물을 우선 대체하거나 중단할 필요성이 있음을 보여준다.
2.4. 고령에서 항콜린제의 사용시 고려사항과 대체약물
고령에서 과민성방광 치료를 위한 항콜린제들 중 인지기능에 영향이 적은 약물을 구분하여 사용하면 안전성을 확보 할 수 있다는 연구들이 많았다. 근거로는 약물의 BBB (blood-brain barrier) 투과성의 차이와 뇌 세포에서 무스카리닉 수용체(M1) 선택성 차이를 제시하고 있다. Oxybutynin과 tolterodine은 lipophilic molecules로 BBB 통과가 상대적으로 쉽고 무스카리닉 수용체 선택성이 없어 M1 수용체에 작용하여 인지기능에 영향을 주기 쉬울 것이라 한다 [13]. 하지만 동물 실험 논문에 근거를 둘 수밖에 없는 한계가 있다. 인간 대상 연구는 대부분 소규모 연구로 인지기능평가도 MMSE나 MoCA 같은 스크리닝 도구에 근거를 두고 있어 한계를 가지고 있다. 이러한 연구들에 근거하여 LUTS-FORTA라는 전문가 합의 과정을 이용한 약물 권고 등급을 발표하여 노인에서 약물 처방에 참고할 수 있도록 하였다 [14]. 과연 비뇨의학과에서는 모두 3점으로 분류된 항콜린제를 구분하여 3.1점 또는 3.8점으로 나눌 수 있을 지에 대해서는 의문을 가질 필요가 있겠다. 만약 가능하다면 노인 임상 연구 근거가 있는 Fesoterodine, Solifenacin, Trospium이 우선 고려대상이 되어야 하며 Oxybutynin과 tolterodine은 제외하는 것이 좋겠다. 최근 연구에서는 type2 당뇨가 있는 환자에서 모든 항콜린제는 BBB 투과성이 증가하여 인지기능저하를 일으킬 수 있어 주의를 요한다고 하며, 이러한 BBB 투과성이 증가할 수 있는 질환으로 multiple sclerosis, type 2 diabetes mellitus, Parkinson disease, and Alzheimer’s disease등이 있다 [15].
대체 약물로는 현재 항콜린제 처방률을 넘어선 Mirabegron (b3-agonist, 50mg)이 있으며 노인 인지기능 관련하여 소규모 연구가 보고되었다. 65세 이상 무작위 위약 대조군 연구로 12주 후 MoCA 수치를 비교하였고 두 군에서 차이를 보이지 않았다 [16]. 또한 저용량을 사용할 수 있는 Propiverine 10mg, Solifenacin 2.5mg도 mirabegron으로 효과가 부족하다면 병합요법으로 고려할 수 있겠다.
3. 결론
1)인지기능 평가를 위해 MMSE-K 도구를 사용한다.
2)항콜린약물부담을 파악하기 위해 KABS를 참고한다. 흔히 사용하는 약물을 미리 파악하여 실제 환자의 다약물복용에 적용하고 대체 또는 중단을 권유한다(예 1세대 항히스타민제->2세대 항히스타민제, H2-blocker ->PPI 제제 등).
3)인지기능이 정상인 경우 항콜린제를 사용 할 수 있고 Fesoterodine, Solifenacin, Trospium이 우선 고려대상이 되어야 하며 Oxybutynin과 tolterodine은 제외하는 것이 좋다.
4)인지기능저하가 의심되거나 2형 당뇨 환자는 항콜린제 사용을 피하고 Mirabegron을 사용한다.
5)Mirabegron의 효과가 부족한 경우 저용량 항콜린제(Propiverine 10mg;BUP4®, Solifenacin 2.5mg; ACARE® 반알) 병용요법을 고려한다.
